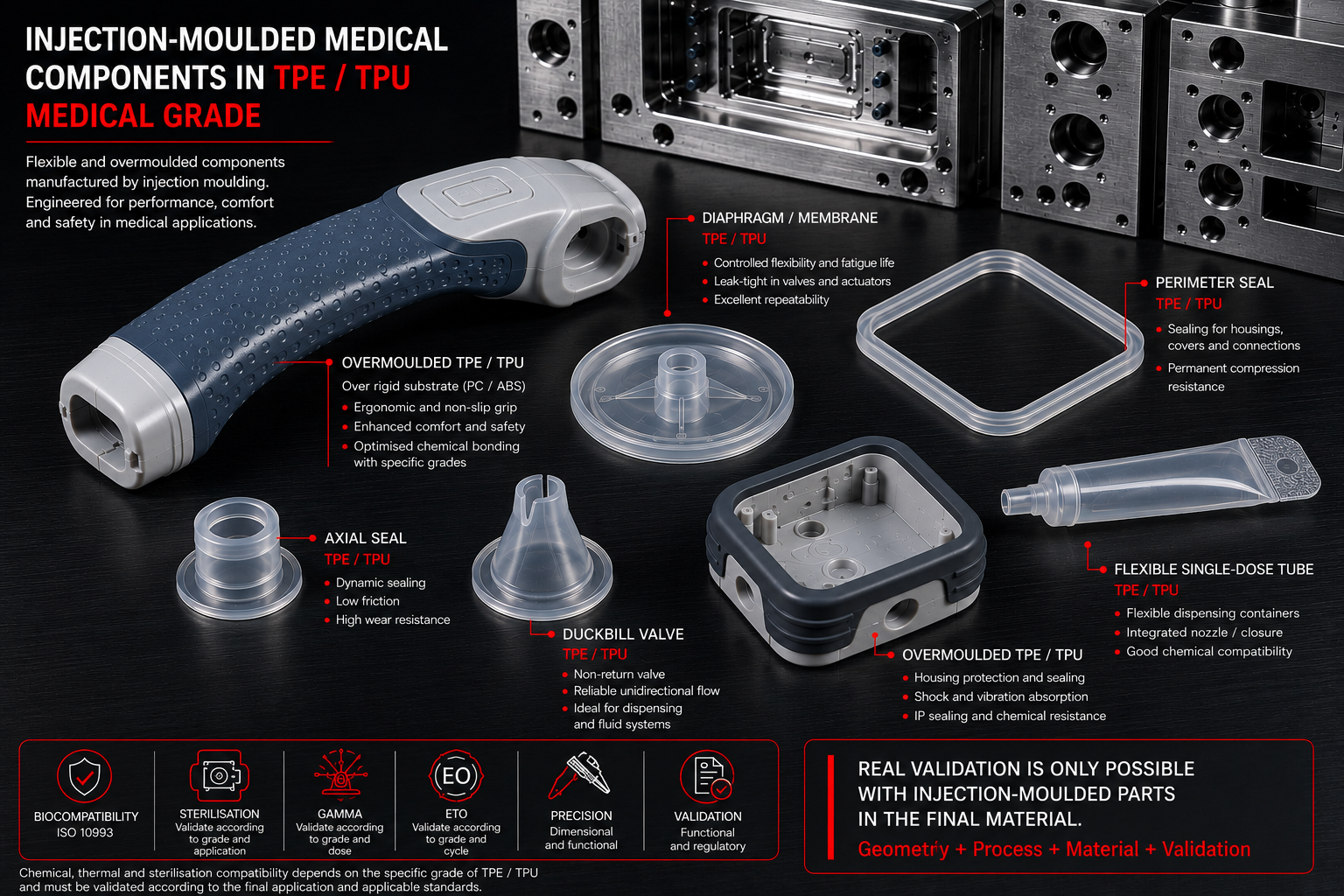
Thermoplastic elastomers (TPE, TPU, TPV, PEBA) are increasingly used in medical devices: ergonomic grips, valves, membranes, tactile interfaces, seals, overmoulded assemblies and patient-contact components. Yet many projects are still validated using rigid prototypes, 3D printing or substitute materials that do not reproduce the real behaviour of the final component. When a product moves from a rigid thermoplastic to an elastomer, it is not just the material that changes — the process, the mould, the validation strategy and part of the regulatory risk change too.

When the final component uses a medical-grade elastomeric material, variables emerge that can only be assessed through injection moulding with the production material:
- ✔ Real demoulding behaviour
- ✔ Processed Shore hardness
- ✔ Shrinkage and elastic recovery
- ✔ Overmoulding adhesion
- ✔ Sterilisation compatibility
- ✔ Functional and regulatory validation
The common mistake: validating an elastomer with rigid-part logic
For rigid materials — PC, ABS, PA66, POM — early validation typically focuses on geometry, tolerances, assembly, interferences and surface finish. The part fills, solidifies and holds its shape. Uncertainties are usually around shrinkage, warpage or cosmetics.
With a medical TPE, the situation changes. Elasticity introduces phenomena that do not exist in rigid parts: elastic recovery, deformation during ejection, cavity stickiness, thermal sensitivity, strain-rate dependency, functional variation by Shore hardness and interaction with sterilisation.
A rigid prototype validates shape. An injection-moulded prototype validates behaviour.
First challenge: demoulding in TPE is functional, not just geometric
In rigid materials, insufficient draft typically causes higher ejection force, surface marks or tool wear. In TPE the problem changes: the part deforms to release and must then recover its geometry.
A moderate undercut that would be acceptable in ABS can lead to permanent deformation, ejection marks, local tearing, stress whitening, sticking or functional distortion.
This is particularly common in:
- Overmoulded components: handles, ergonomic grips, anti-slip surfaces
- Flexible elements: membranes, valves, sealing lips, soft clips
- Tactile interfaces: diagnostic equipment, haptic elements, handheld devices
Real demoulding behaviour can therefore only be assessed when the part is manufactured by injection moulding with the production material.
Second challenge: Shore hardness depends on the process
Many project files specify "TPU 70A" or "TPE 50 Shore A" and assume that property is validated. Not necessarily. Functional hardness depends on the process: melt temperature, residence time, injection speed and pack pressure all affect the final result.
In medical devices, small deviations matter. A variation of a few Shore points can affect:
- Sealing: leak-tightness, insertion force, valve closure
- Ergonomics: tactile feel, grip, comfort
- Mechanical function: stiffness, displacement, elastic recovery
Hardness must therefore be validated on processed parts, not solely on material data sheets.
Third challenge: TPE has process memory
Thermoplastic elastomers are viscoelastic materials. Their response depends on time, temperature, strain rate and thermal history. Two geometrically identical parts can behave differently.
This affects: compression, stress relaxation, recovery, tactile feel and functional response.
Flexible 3D printing does not reproduce flow lines, packing, orientation, real shrinkage or the thermal history of injection moulding. A printed TPU is therefore not equivalent to an injection-moulded one.
Overmoulding in medical devices
Many medical devices combine PC + TPE, ABS + TPU or PA + technical elastomer. The challenge here is no longer the individual part — it is the interface between materials.
Adhesion in medical overmoulding depends on: chemical compatibility, process temperature, surface condition, geometry and coating thickness.
A rigid prototype can validate assembly, but not:
- Real adhesion between substrates
- Peel strength
- Interface ageing
- Delamination under thermal cycling
- Stability after sterilisation
These failures tend to surface late — often only at the pilot mould stage or even during industrial validation.
Sterilisation problems in medical TPE
Here the risk goes beyond the technical and becomes documentary. Not all elastomers tolerate sterilisation methods equally:
- Autoclave: 121 °C — saturated steam
- EtO: ethylene oxide
- Gamma: ionising radiation
Stability depends on the specific material listed in the technical file — not on the substitute, not on the printed prototype, not on a generic TPU. If validation is carried out with alternative materials, the team still does not know the hardness changes, ageing behaviour, deformation, functional stability or real compatibility with the chosen sterilisation method.
And the discovery comes late: during biocompatibility testing, sterilisation or industrial transfer.
Which medical devices use TPE and TPU?
Medical-grade thermoplastic elastomers commonly appear in:
- Patient contact: grips, handles, soft surfaces, ergonomic interfaces
- Sealing: valves, membranes, gaskets, flexible lips
- Diagnostics: portable equipment, tactile interfaces, technical overmouldings
- Consumables: connectors, transfer systems, flexible disposable components
Rigid prototype vs injection-moulded prototype in TPE: what each one actually validates
The table below summarises what can and cannot be validated with each prototyping technology in projects involving TPE in medical devices:
| Technology | Geometry | Ergonomics | Shrinkage | Actual Shore | Sterilisation | Overmoulding |
|---|---|---|---|---|---|---|
| Flexible SLA | Yes | Partial | No | No | No | No |
| TPU 3D printing | Partial | Partial | No | No | No | No |
| Vacuum casting | Yes | High | No | Partial | No | No |
| P2P injection-moulded prototype | Yes | Yes | Yes | Yes | Yes | Yes |
When the goal is to validate the process — not just the shape — rapid tooling, a pilot mould or bridge tooling provides information that no other technology can deliver.
Functional validation with production material
When the prototype uses the actual production material, the team obtains:
- Process validation: real shrinkage, real fill, weld lines, ejection behaviour
- Functional validation: processed Shore hardness, tactile feel, elasticity, recovery
- Industrial validation: overmoulding, adhesion, cycle behaviour, demoulding
- Regulatory validation: sterilisation, biocompatibility, testing on representative parts
At that point the prototype stops being a mock-up and becomes a risk-reduction tool.
The question that changes the project: Does the validation protocol include parts injection-moulded with the registration material? If the answer is no, the first batch from the production mould remains the moment when demoulding problems, Shore deviations, adhesion failures and sterilisation incompatibilities will surface. In medical devices, that discovery does not only affect cost — it affects the validation schedule, documentation and regulatory submission.
P2P prototypes allow injection-moulded prototypes to be produced using the production material, along with pilot moulds, bridge tooling, technical overmoulding and short runs for functional validation prior to industrialisation — particularly in projects involving TPE · TPU · TPV · PEBA · overmoulding · medical devices · technical elastomers.
Frequently asked questions about medical TPE
Can a medical TPE component be validated using 3D printing?
Only partially. 3D printing validates geometry, ergonomics and fit, but typically does not reproduce the shrinkage, rheological behaviour or processed Shore hardness of the component injection-moulded with the production material.
When should an injection-moulded prototype be used?
Whenever the following must be validated: production material, overmoulding, sealing, sterilisation or elastomeric function. In these cases it is the only way to obtain representative data before the pilot mould or production mould.
Is a 3D-printed TPU equivalent to an injection-moulded one?
No. The thermal history and morphology are different. Functional behaviour can change significantly in critical parameters such as processed Shore hardness, elasticity and elastic recovery.
What risks arise when moving directly to the production mould with a medical TPE component?
The most common are: demoulding deformation, Shore hardness deviations, adhesion failures, sterilisation incompatibility and dimensional changes. In medical devices, that discovery also affects the validation schedule, documentation and regulatory submission.